One Dentist or Two? Oral Surgeon vs Dentist for Dental Implants, and Why Coordination Matters More.
2026-06-15
If you've started researching dental implants, you've probably run into a confusing fork: should an oral surgeon place your implant, or a periodontist, or a general dentist? Nearly every article frames the decision that way — which specialist is most qualified to put the post in your jaw.
It's the wrong question. Or at least, it's the second question.
The first one is this: how many providers will your case pass through, and who is accountable for the whole result? Because the most common way an implant case goes wrong isn't a surgeon placing the post badly. It's the handoff — the gap between the person who placed the implant and the person who builds the tooth that goes on top of it. That gap is where coordination fails, where aesthetics become an afterthought, and where, when something doesn't fit, no one will own it.
Oral surgeon vs dentist for dental implants: how the case is usually split
An implant has three parts: the post placed in the bone, the abutment that connects to it, and the crown — the visible tooth. Getting all three right takes two distinct skill sets: surgery and restoration.
In the standard model, those skills live in two different offices. An oral surgeon or periodontist places the implant. Months later, after healing, you return to your general dentist or a prosthodontist to have the crown designed and attached. This is so routine that most patients don't question it — it's simply how implants are usually done.
Here's what that model quietly accepts: the surgeon who places your implant is focused on the surgery, not on the final tooth. The implant goes where the bone is most cooperative. Then the restorative dentist inherits whatever position the implant ended up in and builds a crown to accommodate it. The tooth is designed around the surgery, instead of the surgery being planned around the tooth.
When the bone is generous and the case is simple, this works out fine. When it isn't — a front tooth in the smile zone, an angle that complicates the crown, a soft-tissue result that doesn't look natural — the seams start to show. And the two offices each did their part correctly, so neither is responsible for the part that didn't work: the whole.
The handoff is where cases fail
In our experience, the implant itself usually integrates with the bone. When an implant case disappoints, the cause is more often coordination than the surgery:
- A crown that never quite fits because the implant was angled for surgical ease, not restorative fit.
- An aesthetic result that looks like an implant — grey showing through the gum, the wrong proportion, a tooth that doesn't match its neighbors — because the person who placed it wasn't designing for appearance.
- A loose component or a problem months later, where the surgeon says it's the crown and the restorative dentist says it's the placement, and the patient is left in between making appointments at two offices.
That last scenario is one of the most common reasons patients seek a second opinion. The case isn't catastrophically broken. It's that no single person planned it as one thing, and now no single person owns fixing it.
What changes when one clinician does the whole case
The alternative is straightforward: one clinician plans and executes both the surgery and the restoration, against one plan, from the start.
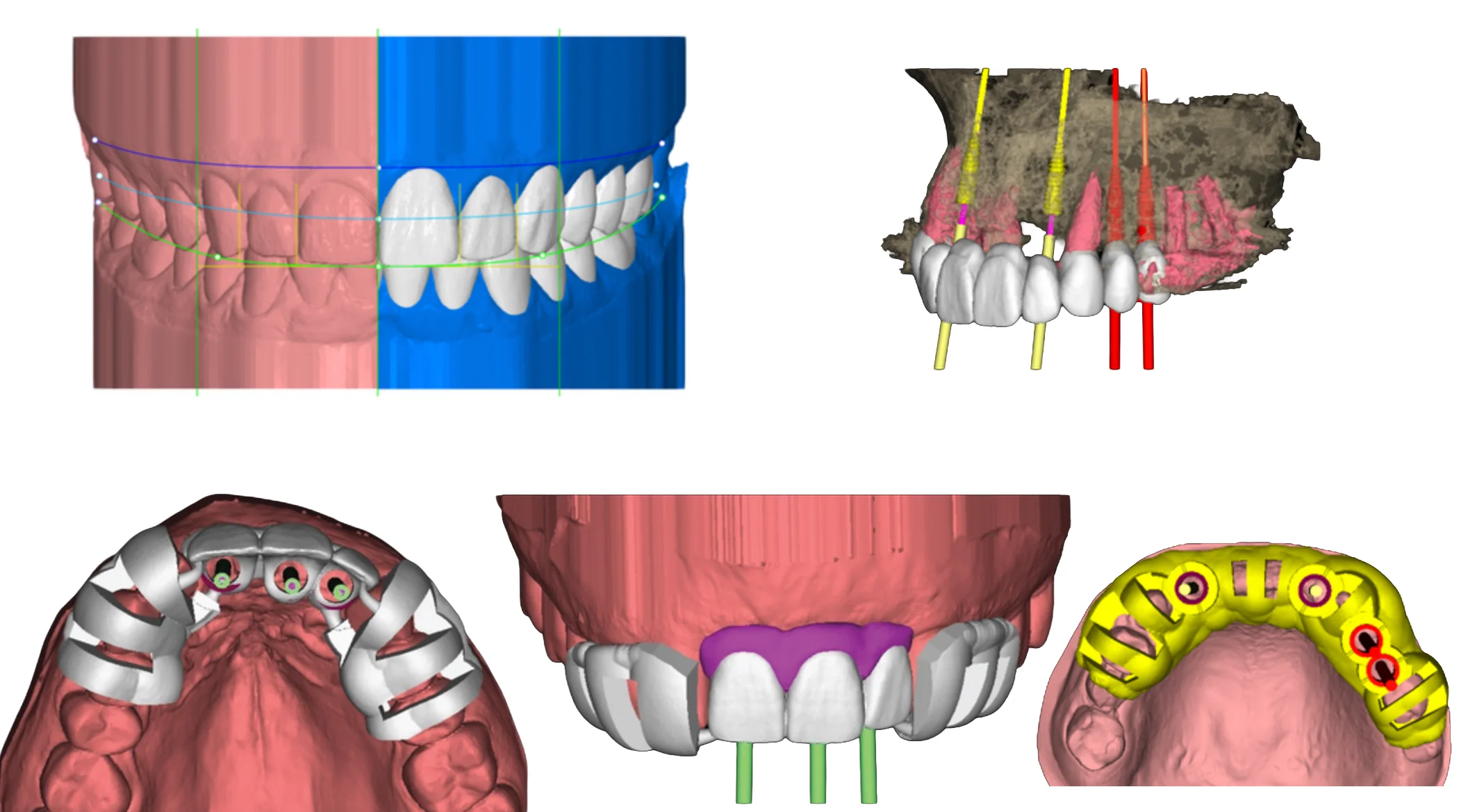
When the same person is responsible for the final tooth and the implant beneath it, the order of planning flips. The finished smile is designed first. The implant position is then derived from where the tooth needs to be — placed to serve the restoration, not just the bone. The surgery becomes a step in building the tooth, rather than a separate event the restoration has to work around afterward.
It also means accountability lives in one place. There's no handoff to fall through, no second office, no diagnostic finger-pointing if something needs adjusting. One person planned it; one person answers for it.
This requires a clinician credentialed in both disciplines, which is uncommon — most dentists are trained in one side or the other, which is exactly why the split model exists. It's the default because dual qualification is rare, not because two offices produce a better result.
How this works at Viva Smile
At Viva Smile in Granada Hills, implant cases are planned and performed by one clinician, Dr. Karen Baghdasaryan, who holds credentials in both sides of the work:
- The surgical side: Associate Fellow of the American Academy of Implant Dentistry (AFAAID) — a credential requiring 600 hours of implant training and examination before a specialist panel.
- The restorative side: Accredited Member of the American Academy of Cosmetic Dentistry (AAACD) — a designation held by fewer than 350 dentists worldwide, earned through documented cosmetic casework judged by a peer panel.
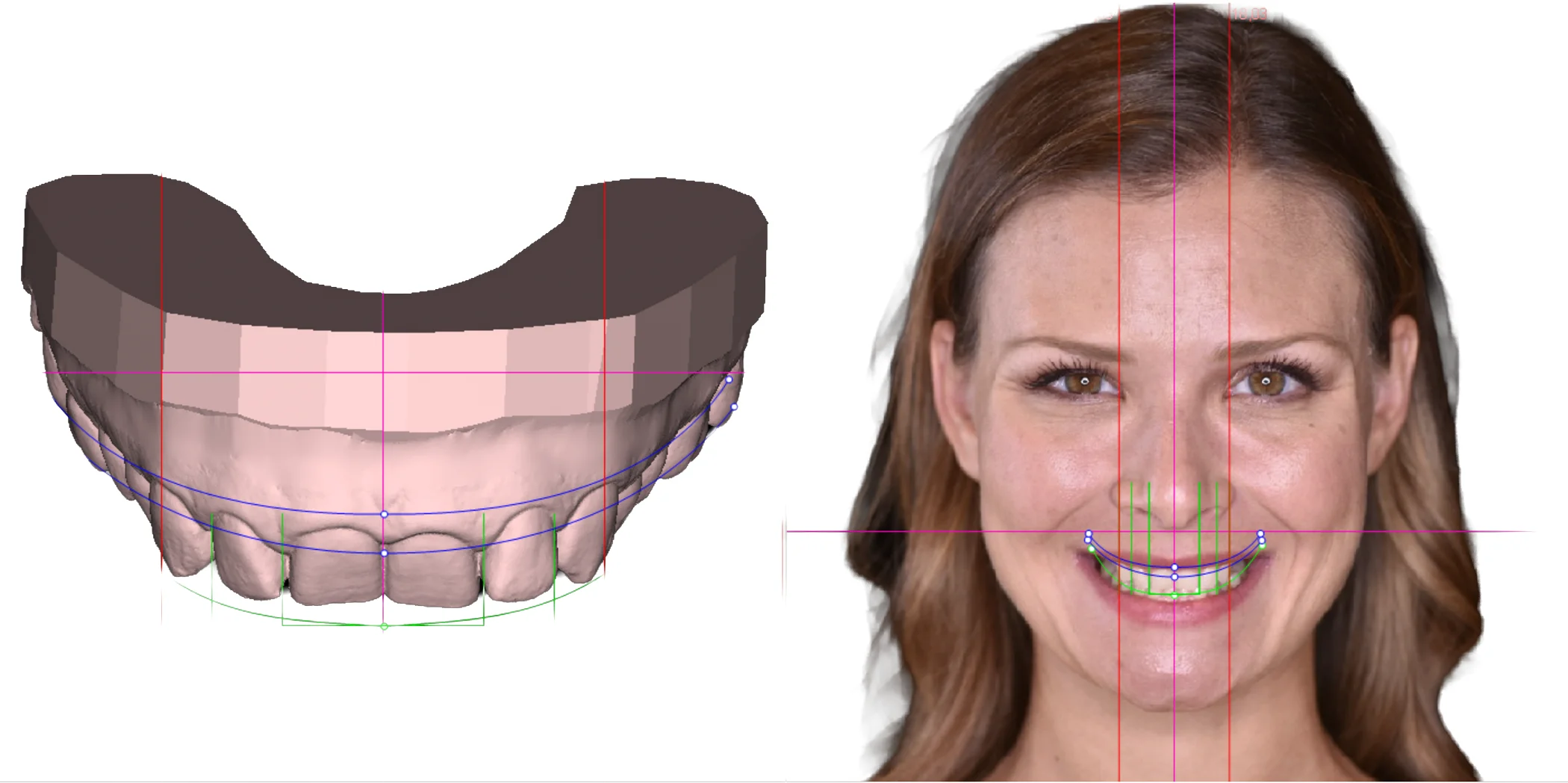
Every case is planned through the Digital Smile Design protocol: the final result is designed first, and the implant placement is guided to serve that design. For straightforward single implants and complex full-arch reconstructions alike, the surgery and the restoration are one continuous plan under one clinician.
This is also why a particular kind of patient ends up here: the one whose implant was placed elsewhere and went wrong. A loose crown, a result that never looked right, a component that failed with no clear owner. Resolving cases that fell through someone else's handoff is regular work at this practice, not an exception.
Who should place your dental implant: periodontist, oral surgeon, or one integrated clinician?
Here's the honest framing, including where the conventional answer still holds:
The split model is fine when your case is simple, your bone is healthy, the tooth isn't in the visible smile zone, and your surgeon and restorative dentist genuinely coordinate. Plenty of cases fit this description and turn out well.
Integrated care matters most when the tooth is in the cosmetic zone, the case is complex (full-arch, significant bone loss, bite reconstruction), aesthetics are a priority, or a previous implant case has already gone wrong. These are the cases where the handoff does the most damage and where one accountable clinician makes the biggest difference.
If you take one thing from this: when you're evaluating implant providers, don't only ask about their surgical credentials. Ask how many providers your case will involve, whether the implant position is planned around the final tooth, and who is accountable if something needs adjusting later. The answers tell you more about your result than the choice between a surgeon and a periodontist.
Frequently asked questions
Can one dentist really do both the surgery and the crown? Yes, if they're credentialed in both. It's uncommon because most dentists train in one side — surgery or restoration — not both. A clinician with both qualifications can plan and complete the full case in one place.
Is an oral surgeon more qualified than a dentist to place implants? For the surgical step in isolation, an oral surgeon has deep surgical training. But implant success depends on more than placement — it depends on the implant being positioned to serve the final tooth, which requires restorative planning too. The strongest outcomes come from cases where both are planned together, by genuinely coordinated providers or by one clinician trained in both.
Why do most implant cases involve two providers? Because dual qualification in both implant surgery and cosmetic restoration is rare. The two-provider model is the default born of that reality — not evidence that splitting the case produces a better result.
What's the risk of having two different providers? The handoff between them. The implant can be placed for surgical convenience rather than restorative fit, aesthetics can become an afterthought, and if a problem arises later, accountability can fall into the gap between the two offices.
I had an implant placed elsewhere and something's wrong. What now? This is one of the most common reasons patients come to us. Bring your records if you have them. A dental exam will show exactly what's going on — whether it's the placement, the crown, or the connection between them — and what it takes to resolve it.
How do I start if I'm considering an implant? A dental exam — $150, covered at 100% by most PPO dental insurance plans — includes the X-rays and 3D scans needed to plan your case properly. You'll leave knowing what your case involves and what it costs, with no decision required on the day.
The bottom line
The implant debate is usually framed as a contest between specialists. The more useful question is how many hands your case passes through and who owns the whole result. A case planned and completed by one clinician — with the implant positioned to serve the final tooth, and one person accountable from surgery through restoration — removes the handoff where most implant cases quietly go wrong.
If you're weighing an implant, or living with one that didn't turn out right, start with a dental exam. It's $150, mostly covered by most PPO insurance, and you'll get an honest read on your situation. Book online or call (818) 900-2800. A free Zoom consultation with Dr. Baghdasaryan is also available if you'd like to talk it through first — though the specifics of your case will ultimately need X-rays to answer.